The Malaysian Government will send 20.9 million medical rubber gloves to five African nations that are affected by the deadly Ebola virus outbreak.
Malaysia will send 11 containers, each holding 1.9 million medical rubber gloves.
Liberia, Sierra Leone and Guinea will each receive three containers; Nigeria and the Democratic Republic of Congo will each receive one container.
Posted Date 09-15-2014
More than 40,000 types of commercial products are made from natural rubber latex (NRL), an extract of the Pará rubber tree. Valued for its desirable properties, NRL is used in numerous products in the medical industry and elsewhere, including latex gloves. However, out of more than 200 proteins contained within NRL, 13 are known to be allergens.
Posted Date 04-01-2011
Disposable nitrile, natural latex, and vinyl gloves, often referred to as thin-mil gloves, are used in a variety of distinct applications. Understanding the truths about glove performance is important in selecting the right glove for each application.
Posted Date 04-01-2010


Like any healthcare professional, those working in small medical offices know that protection against blood and other bodily fluids is essential for preventing disease and the transmission of illnesses. Medical gloves are one of the first lines of defense.
In general, medical gloves are made of polymers like latex, nitrile rubber, vinyl, neoprene and polyisoprene. Each material has its own strengths and benefits and is best suited for specific types of work. Before you place an order, it’s important to know which type of glove will best meet your needs.
1. What is Ebola virus disease?
Ebola virus disease (formerly known as Ebola haemorrhagic fever) is a severe, often fatal illness, with a death rate of up to 90%. The illness affects humans and nonhuman primates (monkeys, gorillas, and chimpanzees).
If you have a latex allergy, you could be in danger of having an allergic reaction at your local family restaurant. Recent studies have found that latex gloves worn during food preparation can shed latex proteins into the food in amounts large enough to cause reactions.
The studies were a result of multiple reports from latex-allergic individuals who claimed that they had experienced allergic reactions from eating food at restaurants that used latex gloves. One study done at the Guthrie Research Institute found that fingerprints of latex proteins were detectable on cheese and lettuce that were handled with latex gloves.

Q. Can staff wear gloves instead of cleaning their hands?
A. No. Gloves are not a substitute for handwashing or hand disinfection. Glove usage should be appropriate for the task in hand and removed at the end of the task for which they were worn.
Gloves can protect both patients and healthcare workers from exposure to infectious agents that may be carried on hands (Duckro et al 2005). As part of standard precautions, they are used to prevent contamination of healthcare workers’ hands when (Siegel et al 2007):
Evidence and different considerations on glove use
It is widely recommended that health-care workers (HCWs) wear gloves for
two main reasons: (i) to prevent microorganisms which may be infecting,
commensally carried, or transiently present on HCWs’ hands from being
transmitted to patients and from one patient to another; (ii) to reduce the
risk of HCWs themselves acquiring infections from patients.
TUESDAY, June 16 (HealthDay News) -- Holes in surgical gloves increase the risk of surgical site infection among patients who aren't given antibiotics before their surgery, Swiss researchers say.
In procedures lasting more than two hours, the rate of glove perforations ranges from 8 percent to 50 percent, according to a study published in the June issue of the Archives of Surgery.
Posted Date 05-16-2009
Summary: Use this checklist to choose the appropriate type of protective glove for your job. The Glove Selection Chart also provides advantages and disadvantages for specific glove types. This guidance was prepared for laboratory researchers but may also be helpful for other people working with hazardous materials.
This second edition of the ADA Guidelines for Infection Control incorporates a number of changes that have arisen since the publication of the first edition in 2008, including the release in October 2010 of the National Health and Medical Research Council (NHMRC) Australian Guidelines for the Prevention and Control of Infection in Healthcare . It is the intention of the Australian Dental Association Inc. (ADA) that these infection control guidelines will be updated every three years to ensure that they remain aligned to the evidence base of infection control.
THE FIRST GLOBAL PATIENT SAFETY CHALLENGE
Clean Care is Safer Care
GLOVE USE (technical)
Evidence and different considerations on glove use
It is widely recommended that health-care workers (HCWs) wear gloves for two main reasons: (i) to prevent microorganisms which may be infecting, commensally carried, or transiently present on HCWs’ hands from being transmitted to patients and from one patient to another; (ii) to reduce the risk of HCWs themselves acquiring infections from patients.
The effectiveness of gloves in preventing contamination of HCWs’ hands and helping to reduce transmission of pathogens has been confirmed in several clinical studies.
Nevertheless HCWs should be informed that gloves do not provide complete protection against hand contamination. Bacterial flora colonizingpatients may be recovered from the hands of up to 30% of HCWs whowear gloves during patient contact. In such instances, pathogens presumably gain access to the caregivers’ hands via small defects in gloves or bycontamination of the hands during glove removal.
The impact of wearing gloves on adherence to hand hygiene policies has not been definitively established, since published studies have yielded contradictory results. Several studies found that HCWs who wore gloves were less likely to cleanse their hands upon leaving a patient’s room. In contrast, other studies proved the direct opposite. The recommendation to wear gloves during an entire episode of care of a patient undergoing isolation precautions could actually lead to HCWs missing opportunities for hand hygiene
Use of gloves
Gloves should be worn during all patient-care activities that may involve exposure to blood or body fluids contaminated with blood. In addition, gloves should be worn in activities that include contact with potentially infectious material other than blood, such as mucous membranes, and non-intact skin or during outbreak situations, as recommended by specific requirements for Personal Protective Equipment (PPE).
The unnecessary use of gloves in situations when their use is not recommended represents a waste of resources without necessarily leading to a reduction of cross-transmission and may also result in missed opportunities for hand hygiene.
It is important that HCWs are able to correctly select the most appropriate type of gloves to be worn and to differentiate between specific clinical situ ations when gloves should be worn and changed and those where their use is not recommended (see pyramid overleaf).
Glove reprocessing must be strongly discouraged and should be avoided, even if it is common practice in many health-care settings in developing countries where glove supply is limited. At present no standardized, validated and affordable procedure for safe glove reprocessing exists. Every possible effort should be made to prevent the occurrence of glove reuse in health-care settings. This includes educational activities to reinforce the need to reduce inappropriate glove use, purchasing good quality disposable gloves and replenishing stocks in time. Further research is needed to identify a standardized glove reprocessing procedure, to evaluate the integrity of different glove material when exposed to different products used for hand antisepsis or handwashing (e.g. alcohol, chlorhexidine, or iodine solutions) and to develop a valid evaluation process for settings practicing or planning the reprocessing of gloves, in order to minimize this practice.
Key messages for glove use:
Recommendations on glove use:
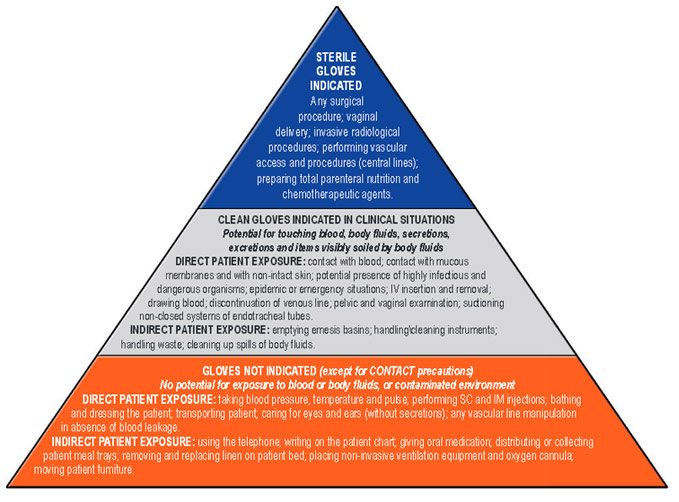
Gloves must be worn according to STANDARD and CONTACT PRECAUTIONS. The pyramid details some clinical examples in which gloves are not indicated, and others in which clean or sterile gloves are indicated. Hand hygiene should be performed when appropriate regardless of these indications for glove use.
Glove Selection Guide
Summary: Use this checklist to choose the appropriate type of protective glove for your job. The Glove Selection Chart also provides advantages and disadvantages for specific glove types. This guidance was prepared for laboratory researchers but may also be helpful for other people working with hazardous materials.
What to do |
How to do it |
| 1. Identify the hazards of the material(s) you'll be working with. | 1. Base selection of glove type and material on the type of exposure and nature of the hazard. Some chemicals can easily penetrate gloves that work very well for other chemicals. Consider these factors:
2. Read the Safety Data Sheets (SDSs) for each chemical involved. |
| 2. Determine if you'll have incidental or extended contact with the hazardous materials. | 1. Incidental contact (little or no direct contact with the hazardous material) includes these situations:
If you will have incidental contact, go to the Step 3. 2. Extended contact includes these situations:
If you will have extended contact, go to Step 4. |
| 3. For incidental contact, follow these selection guidelines. |
1. Type of glove: Disposable, surgical-type gloves are appropriate for incidental contact. 2. Nitrile gloves are preferred over latex because of their chemical resistance, their tendency to visibly rip when punctured, and to prevent possible latex allergies.
3. Disposable glove usage:
|
| 4. For extended contact, follow these guidelines. |
1. Type of glove: More substantial gloves are required for extended use.
2. Reusable glove usage: Many gloves intended for extended contact are reusable.
|
| 5. Dispose of used and damaged gloves according to whether or not they're contaminated with a hazardous material. | 1. Follow the appropriate guidelines below:
ALWAYS wash your hands after removing gloves. Watch a short video on correct hand washing. |
Once selected, glove use requirements for your lab should be posted in your Chemical Hygiene Plan flipchart under the Standard Operating Procedures section.
Questions about glove selection?
Please contact the Office of Environment, Health and Safety at 642-3073 or [email protected].
Glove Comparison Chart |
| Summary: Consult this chart for an overview of commonly used glove types for laboratory use and their general advantages and disadvantages. |
Glove material |
Intended use |
Advantages and disadvantages |
Example Photos |
| Latex (natural rubber) | Incidental contact |
|
 |
| Nitrile | Incidental contact (disposable exam glove)
Extended contact (thicker reusable glove) |
Good alternative for those with latex allergies. |
 |
| Butyl rubber | Extended contact |
|
 |
| Neoprene | Extended contact |
|
 |
| Norfoil | Extended contact |
|
 |
| Viton | Extended contact |
|
 |
| Polyvinyl chloride (PVC) | Specific use |
|
 |
| Polyvinyl alcohol (PVA) | Specific use |
|
 |
| Stainless steel
Kevlar Leather |
Specific use | Cut-resistant gloves.
Sleeves are also available to provide protection to wrists and forearms. (If potential for biological or chemical contamination: wear appropriate disposable gloves on top of your cut-resistant gloves and discard after use). |
|
| Cryogenic Resistant Material
Leather |
Specific use | For use with cryogenic materials.
Designed to prevent frostbite. Note: Never dip gloves directly into liquid nitrogen. |
 |
| Nomex | Specific use | For use with pyrophoric materials.
Consider wearing a flame-resistant glove such as a Nomex 'flight' glove with a thin nitrile exam glove underneath. |
 |







